
Do you ever feel “wrestless” or “nervous” out of the blue? Perhaps you have a feeling which you try to ignore, suggesting that you are not as good as others, that there is something broken about you. You may either seek to hide this “truth” or you feel ashamed “knowing” that others can tell you are broken?
This is the heart of struggles in individuals with Complex-PTSD. Complex PTSD (C-PTSD) is a psychological (and even visceral) condition that arises from prolonged or repeated exposure to traumatic events, often during formative periods of childhood or in situations where escape is difficult, such as in abusive relationships or on-going emotional or physical neglect. At the heart of childhood C-PTSD, an attachment disruption occurs, as often a child’s caregiver is also the source of their trauma. While C-PTSD is not yet officially recognized in the DSM-5, it is increasingly acknowledged within the global mental health community, particularly through the ICD-11, which now includes it as a distinct diagnosis. This article will provide an overview of what C-PTSD is, how it differs from traditional PTSD, and explore evidence-based treatment approaches for healing.
It is worth noting that while the DSM-5 did not include this diagnosis specifically, it did add some new symptom sets to broaden the diagnosis of PTSD, so that those presenting with C-PTSD can be captured in the nuances of such additions. Critics argue that this is not enough for diagnostic clarity and effective treatment planning.
What is Complex PTSD?
Complex PTSD refers to a form of trauma-related disorder that arises from long-term or repeated exposure to trauma, often in situations where individuals feel trapped or powerless. These might include experiences such as childhood emotional or physical abuse or neglect, witnessing chronic domestic violence, prolonged emotional or physical neglect, or living in high crime areas.
While post-traumatic stress disorder (PTSD) can develop from a single traumatic event (such as witnessing a death), C-PTSD typically stems from ongoing, chronic trauma. C-PTSD often involves traumatic events that were relational in nature. For example, having a father who is often criticizing you, telling you are “worthless” or that he wishes you were not born. Or having a mother who is often under the influence of substances, acting unpredictable, impulsive and risky; putting a child in a constant state of fear of “what can happen when mom is drinking”.
A recent training I attended by Bessel Van der Kolk, who is considered one of the leading trauma experts in psychology, shared his research showing the critical differences between being a child who experiences trauma within their own family versus being an adult who gets in an accident or is assaulted, in that the former changes a person’s sense of themselves. Rather than having a core belief of “I am capable and safe, but I went through something scary”, the core belief is “I am defective and damaged, and bad things happen to me because the world is not safe for me.” This explains why therapy for complex-trauma is often much longer than treatment for more typical PTSD, with much of the focus on the healing power of the therapeutic relationship rather than just the interventions for processing the trauma.
Some key symptoms of C-PTSD include:
– Re-experiencing the Trauma: This may include flashbacks, intrusive memories, or nightmares related to the traumatic events.
Avoidance: A person may avoid people, places, or activities that remind them of the trauma.
– Negative Alterations in Mood and Cognition: This includes feelings of shame, guilt, hopelessness, or emotional numbness, and difficulty in forming positive relationships.
– Hyperarousal: Individuals may feel constantly on edge, with symptoms like irritability, difficulty sleeping, and exaggerated startle responses.
– Dissociation: Individuals may experience a sense of detachment from themselves or the world around them.
– Disturbance in Self-Identity: A person may experience feelings of worthlessness, guilt, or a persistent sense of being broken or damaged.
Why is C-PTSD Not Officially in the DSM-5?
Although C-PTSD is increasingly recognized as a distinct form of PTSD, it has not yet been included in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). The DSM-5, published by the American Psychiatric Association, is the primary tool used by clinicians in the United States to diagnose mental health conditions.
Despite strong support from mental health professionals for including C-PTSD as a standalone diagnosis, it was ultimately excluded from the DSM-5. The main reason for this exclusion lies in ongoing debates within the field about the diagnostic criteria for C-PTSD and whether it sufficiently differs from PTSD to warrant a separate category- especially now that the newest DSM added some clusters of symptoms that can better catch C-PTSD in its umbrella.
That said, the International Classification of Diseases, 11th Edition (ICD-11), a globally recognized diagnostic tool used by health professionals worldwide, has formally recognized Complex PTSD as a distinct disorder. The inclusion of C-PTSD in the ICD-11 marks an important milestone in global mental health practice, as it allows clinicians around the world to diagnose and treat C-PTSD more accurately.
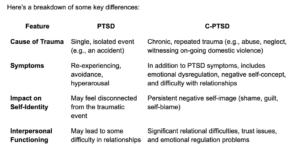
Key Differences Between PTSD and C-PTSD
While PTSD and C-PTSD share several symptoms, there are notable differences. The most significant distinction is the duration and type of trauma experienced. PTSD is typically linked to a single traumatic event (e.g., a car accident, a natural disaster, or an assault), while C-PTSD results from prolonged or repeated trauma, often involving interpersonal or relational harm.
The person responsible for the trauma is crucial in understanding its impact. When children experience complex trauma, it often occurs within the context of caregiver relationships, where abuse or neglect can be more damaging than harm from an outsider. This is because it undermines the child’s fundamental understanding of healthy attachment, distorts their perception of others as safe, and breaks the basic expectation that caregivers will consistently offer love, care, and protection.
Treatment Approaches for Complex PTSD
While the journey toward healing from C-PTSD can be long and challenging, there are several effective therapeutic approaches that can help individuals manage and heal from their symptoms.
Trauma-Focused Therapy for C-PTSD
– Trauma-Focused Cognitive Behavioral Therapy (TF-CBT): This is an adapted version of CBT that specifically targets trauma. It’s particularly effective for people dealing with childhood trauma or sexual abuse.
-EMDR (Eye Movement Desensitization and Reprocessing)
EMDR is a therapeutic approach that helps individuals reprocess traumatic memories by using bilateral stimulation (such as guided eye movements). EMDR helps people integrate traumatic memories and feelings into their broader life narrative, reducing emotional pain and distress.
Other Therapy for C-PTSD
– Dialectical Behavior Therapy (DBT): DBT was originally developed for individuals with borderline personality disorder, but it has shown success in treating emotional dysregulation, which is often a key symptom of C-PTSD. DBT helps clients develop emotional regulation skills, improve interpersonal effectiveness, and enhance distress tolerance.
– Somatic Therapies
Somatic therapies focus on the mind-body connection and are particularly helpful for individuals whose trauma is stored in the body. Techniques such as Somatic Experiencing and Sensorimotor Psychotherapy can help release trauma-related tension, improve emotional regulation, and restore a sense of safety in the body.
– Attachment-Based and Relational Therapy
Since C-PTSD often involves relational trauma, relational or attachment-based therapies can be beneficial and in my opinion, need to be part of the treatment process. These therapies focus on repairing and improving the client’s ability to form secure attachments with others and rebuild a sense of trust and safety.
– Mindfulness and Grounding Techniques
Grounding exercises and mindfulness practices can be incredibly helpful for individuals with C-PTSD, particularly for managing dissociation, anxiety, and hyperarousal. These techniques help clients reconnect with the present moment, stay grounded, and regulate intense emotions.
Conclusion:
Complex PTSD is a deeply impactful condition that arises from prolonged exposure to trauma that is often relational in nature, causing deep relational wounds within an individual and feelings of being “broken” or “damaged”. Though it is not yet included in the DSM-5, the inclusion of C-PTSD in the ICD-11 has helped validate the experiences of those living with this disorder. Fortunately, there are many effective treatment options available that can help individuals heal, regain control over their lives, and restore a sense of hope and safety.
If you are struggling with symptoms of C-PTSD, seeking therapy with a trained professional can be the first step toward healing. While therapy tends to take longer for C-PTSD, since much of the underlying treatment involves having a corrective, stable, and consistent healing relationship with your therapist and then yourself, recovery is possible. You don’t have to walk the path of healing alone.